What'S Posterior Tibial Tendon Dysfunction ?
Overview
Becoming flatfooted can be a real health issue for people. The advice from healthcare experts is to pay attention to foot pain, and when it happens, to seek help right away. In the last 20 years, adult-acquired flatfoot has become a more commonly recognized health issue. The cause is a dysfunction of the ankle tendon that attaches to the bones on the inside of your foot. The function of this posterior tibial tendon (PTT) is to maintain the foot arch and provide strength during push-off when you walk. When the PTT is not functioning correctly, you tend to lose your arch, or become more flatfooted. This problem occurs about three times more often in women than in men, especially after the age of 40. Initially, PTT dysfunction is associated with pain on the inside of the ankle, swelling and sometimes a limp. If left unchecked, the arch appears to collapse and the pain on the inside of the ankle worsens. Eventually, if left unchecked, patients will begin to feel pain on the outside of the ankle, too. 
Causes
Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Perform a structural assessment of the foot and ankle. Check the ankle for alignment and position. When it comes to patients with severe PTTD, the deltoid has failed, causing an instability of the ankle and possible valgus of the ankle. This is a rare and difficult problem to address. However, if one misses it, it can lead to dire consequences and potential surgical failure. Check the heel alignment and position of the heel both loaded and during varus/valgus stress. Compare range of motion of the heel to the normal contralateral limb. Check alignment of the midtarsal joint for collapse and lateral deviation. Noting the level of lateral deviation in comparison to the contralateral limb is critical for surgical planning. Check midfoot alignment of the naviculocuneiform joints and metatarsocuneiform joints both for sag and hypermobility.
Non surgical Treatment
Flatfoot deformity can be treated conservatively or with surgical intervention depending on the severity of the condition. When people notice their arches flattening, they should immediately avoid non-supportive shoes such as flip-flops, sandals or thin-soled tennis shoes. Theses shoes will only worsen the flatfoot deformity and exacerbate arch pain. Next, custom orthotics are essential for people with collapsed arches. Over-the-counter insoles only provide cushion and padding to the arch, whereas custom orthotics are fabricated to specifically fit the patient?s foot and provide support in the arch where the posterior tibial tendon is unable to anymore. Use of custom orthotics in the early phases of flatfoot or PTTD can prevent worsening of symptoms and prevent further attenuation or injury to the posterior tibial tendon. In more severe cases of flatfoot deformity an ankle foot orthosis (AFO) such as a Ritchie brace is needed. This brace provides more support to the arch and hindfoot rather than an orthotic but can be bulky in normal shoegear. Additional treatment along with use of custom orthotics is use of non-steroidal anti-inflammatories (NSAIDS) such as Advil, Motrin, or Ibuprofen which can decrease inflammation to the posterior tibial tendon. If pain is severe, the patient may need to be placed in a below the knee air walker boot for several weeks which will allow the tendon to rest and heal, especially if a posterior tibial tendon tear is noted on MRI. 
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Do You Really Understand Heel Painfulness?
Overview

Heel pain is unlike most body aches and injuries because heels can't be immobilized to rest and recover, at least without considerable inconvenience to the sufferer. Heels can?t be isolated and splinted either ,as body weight will continue to aggravate the condition with every step. Heel pain can be devastating if left untreated, eventually impairing the ability to walk comfortably-or at all. Most Heel Pain comes from tendon problems, though some types can come from bone issues as well.
Causes
While heel pain has many causes, it is usually the result of poor biomechanics (abnormalities in the way we walk). This can place too much stress on the heel bone and the soft tissues attached to it. The stress may result from injury, or a bruise incurred while walking, running or jumping on hard surfaces: wearing poorly constructed footwear or being significantly over weight. Systemic diseases such as arthritis can also contribute to heel pain.
Symptoms
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Heel pain is unlike most body aches and injuries because heels can't be immobilized to rest and recover, at least without considerable inconvenience to the sufferer. Heels can?t be isolated and splinted either ,as body weight will continue to aggravate the condition with every step. Heel pain can be devastating if left untreated, eventually impairing the ability to walk comfortably-or at all. Most Heel Pain comes from tendon problems, though some types can come from bone issues as well.
Causes
While heel pain has many causes, it is usually the result of poor biomechanics (abnormalities in the way we walk). This can place too much stress on the heel bone and the soft tissues attached to it. The stress may result from injury, or a bruise incurred while walking, running or jumping on hard surfaces: wearing poorly constructed footwear or being significantly over weight. Systemic diseases such as arthritis can also contribute to heel pain.
Symptoms
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Precisely What Will Cause Tendonitis In The Achilles ?
Overview
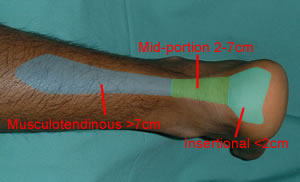 The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
Causes
Achilles tendonitis most commonly occurs due to repetitive or prolonged activities placing strain on the Achilles tendon. This typically occurs due to excessive walking, running or jumping activities. Occasionally, it may occur suddenly due to a high force going through the Achilles tendon beyond what it can withstand. This may be due to a sudden acceleration or forceful jump. The condition may also occur following a calf or Achilles tear, following a poorly rehabilitated sprained ankle or in patients with poor foot biomechanics or inappropriate footwear. In athletes, this condition is commonly seen in running sports such as marathon, triathlon, football and athletics.
Symptoms
Recurring localized pain, sometimes severe, along the tendon during or a few hours after running. Morning tenderness about an inch and a half above the point where the Achilles tendon is attached to the heel bone. Sluggishness in your leg. Mild or severe swelling. Stiffness that generally diminishes as the tendon warms up with use.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose an Achilles injury such as Achilles tendonitis. Occasionally, further investigations such as an Ultrasound, X-ray or MRI scan may be required to assist with diagnosis and assess the severity of the condition.
Nonsurgical Treatment
Treatment will focus on relieving the pain and preventing further injury. Your podiatrist may create shoe inserts or a soft cast to effectively immobilize the affected area for a period of time. (Often, a couple of weeks are needed for the tendon to heal.) Medication can help too. Your podiatrist may recommend or prescribe oral medication.

Surgical Treatment
It is important to understand that surgery may not give you 100% functionality of your leg, but you should be able to return to most if not all of your pre-injury activities. These surgical procedures are often performed with very successful results. What truly makes a difference is your commitment to a doctor recommended rehabilitation program after surgery as there is always a possibility of re-injuring your tendon even after a surgical procedure. One complication of surgical repair for Achilles tendon tear is that skin can become thin at site of incision, and may have limited blood flow.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
Causes
Achilles tendonitis most commonly occurs due to repetitive or prolonged activities placing strain on the Achilles tendon. This typically occurs due to excessive walking, running or jumping activities. Occasionally, it may occur suddenly due to a high force going through the Achilles tendon beyond what it can withstand. This may be due to a sudden acceleration or forceful jump. The condition may also occur following a calf or Achilles tear, following a poorly rehabilitated sprained ankle or in patients with poor foot biomechanics or inappropriate footwear. In athletes, this condition is commonly seen in running sports such as marathon, triathlon, football and athletics.
Symptoms
Recurring localized pain, sometimes severe, along the tendon during or a few hours after running. Morning tenderness about an inch and a half above the point where the Achilles tendon is attached to the heel bone. Sluggishness in your leg. Mild or severe swelling. Stiffness that generally diminishes as the tendon warms up with use.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose an Achilles injury such as Achilles tendonitis. Occasionally, further investigations such as an Ultrasound, X-ray or MRI scan may be required to assist with diagnosis and assess the severity of the condition.
Nonsurgical Treatment
Treatment will focus on relieving the pain and preventing further injury. Your podiatrist may create shoe inserts or a soft cast to effectively immobilize the affected area for a period of time. (Often, a couple of weeks are needed for the tendon to heal.) Medication can help too. Your podiatrist may recommend or prescribe oral medication.
Surgical Treatment
It is important to understand that surgery may not give you 100% functionality of your leg, but you should be able to return to most if not all of your pre-injury activities. These surgical procedures are often performed with very successful results. What truly makes a difference is your commitment to a doctor recommended rehabilitation program after surgery as there is always a possibility of re-injuring your tendon even after a surgical procedure. One complication of surgical repair for Achilles tendon tear is that skin can become thin at site of incision, and may have limited blood flow.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
What Is Pain In The Heel And The Way To Prevent It

Overview
Plantar fasciitis is the most common cause of heel pain. The plantar fascia camera.gif is the flat band of tissue (ligament) that connects your heel bone to your toes. It supports the arch of your foot. If you strain your plantar fascia, it gets weak, swollen, and irritated (inflamed). Then your heel or the bottom of your foot hurts when you stand or walk. Plantar fasciitis is common in middle-aged people. It also occurs in younger people who are on their feet a lot, like athletes or soldiers. It can happen in one foot or both feet.
Causes
Training on improper, hard and/or irregular surfaces as well as excessive track work in spiked shoes, or steep hill running, can stress the plantar fascia past its limits of elasticity, leading to injury. Finally, failure in the early season to warm up gradually gives the athlete insufficient time for the structures of the foot to re-acclimate and return to a proper fitness level for intensive exercise. Such unprepared and repeated trauma causes microscopic tearing, which may only be detected once full-blown plantar fasciitis and accompanying pain and debilitation have resulted. If the level of damage to the plantar fascia is significant, an inflammatory reaction of the heel bone can produce spike-like projections of new bone, known as heel spurs. Indeed, plantar fasciitis has occasionally been refereed to as heel spur syndrome, though such spurs are not the cause of the initial pain but are instead a further symptom of the problem. While such spurs are sometimes painless, in other cases they cause pain or disability in the athlete, and surgical intervention to remove them may be required. A dull, intermittent pain in the heel is typical, sometimes progressing to a sharp, sustained discomfort. Commonly, pain is worse in the morning or after sitting, later decreasing as the patient begins walking, though standing or walking for long periods usually brings renewal of the pain.
Symptoms
The typical presentation is sharp pain localized at the anterior aspect of the calcaneus. Plantar fasciitis has a partial association with a heel spur (exostosis); however, many asymptomatic individuals have bony heel spurs, whereas many patients with plantar fasciitis do not have a spur.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
The initial treatment of plantar fasciitis focuses on reducing pain and inflammation. Resting the affected foot is the most important aspect of this treatment. Other initial treatment may include, aplying ice to the sole of the foot, Anti-inflammatory medications. Gentle stretching of the plantar fascia and Achilles tendon. Physiotherapy. Taping the foot and ankle to provide adequate support and alignment, Wearing supportive footwear with shock-absorbing soles or inserts. Non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Brufen) and diclofenac (Voltaren) are often used to treat plantar fasciitis. It is unclear whether NSAIDs assist in the healing process but they are useful for controlling pain during treatment. If the condition does not respond to initial treatment, a corticosteroid therapy may be recommended. This involves the injection of corticosteroid medication such as hydrocortisone (Solu-Cortef) directly into the affected area in order to treat the inflammation and thus relieve the pain. Night splints to prevent the plantar fascia tightening during sleep may also be recommended at this stage.

Surgical Treatment
In unusual cases, surgical intervention is necessary for relief of pain. These should only be employed after non-surgical efforts have been used without relief. Generally, such surgical procedures may be completed on an outpatient basis in less than one hour, using local anesthesia or minimal sedation administrated by a trained anesthesiologist. In such cases, the surgeon may remove or release the injured and inflamed fascia, after a small incision is made in the heel. A surgical procedure may also be undertaken to remove bone spurs, sometimes as part of the same surgery addressing the damaged tissue. A cast may be used to immobilize the foot following surgery and crutches provided in order to allow greater mobility while keeping weight off the recovering foot during healing. After removal of the cast, several weeks of physical therapy can be used to speed recovery, reduce swelling and restore flexibility.
What Will Cause Pain On The Heel And Ways To Fix It

Overview
Plantar fasciitis is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition every year. Plantar fasciitis occurs when the strong band of tissue that supports the arch of your foot becomes irritated and inflamed. The plantar fascia is a long, thin ligament that lies directly beneath the skin on the bottom of your foot. It connects the heel to the front of your foot, and supports the arch of your foot.
Causes
You are more likely to develop plantar fasciitis if you are Active, sports that place excessive stress on the heel bone and attached tissue, especially if you have tight calf muscles or a stiff ankle from a previous ankle sprain, which limits ankle movement eg. Running, ballet dancing and aerobics. Overweight. Carrying around extra weight increases the strain and stress on your plantar fascia. Pregnant. The weight gain and swelling associated with pregnancy can cause ligaments to become more relaxed, which can lead to mechanical problems and inflammation. On your feet. Having a job that requires a lot of walking or standing on hard surfaces ie factory workers, teachers and waitresses. Flat Feet or High Foot Arches. Changes in the arch of your foot changes the shock absorption ability and can stretch and strain the plantar fascia, which then has to absorb the additional force. Middle-Aged or Older. With ageing the arch of your foot may begin to sag - putting extra stress on the plantar fascia. Wearing shoes with poor support. Weak Foot Arch Muscles. Muscle fatigue allows your plantar fascia to overstress and cause injury. Arthritis. Some types of arthritis can cause inflammation in the tendons in the bottom of your foot, which may lead to plantar fasciitis. Diabetes. Although doctors don't know why, plantar fasciitis occurs more often in people with diabetes.
Symptoms
The classic sign of plantar fasciitis is that the worst pain occurs with the first few steps in the morning, but not every patient will have this symptom. Patients often notice pain at the beginning of activity that lessens or resolves as they warm up. The pain may also occur with prolonged standing and is sometimes accompanied by stiffness. In more severe cases, the pain will also worsen toward the end of the day.
Diagnosis
If you see a doctor for heel pain, he or she will first ask questions about where you feel the pain. If plantar fasciitis is suspected, the doctor will ask about what activities you've been doing that might be putting you at risk. The doctor will also examine your foot by pressing on it or asking you to flex it to see if that makes the pain worse. If something else might be causing the pain, like a heel spur or a bone fracture, the doctor may order an X-ray to take a look at the bones of your feet. In rare cases, if heel pain doesn't respond to regular treatments, the doctor also might order an MRI scan of your foot. The good news about plantar fasciitis is that it usually goes away after a few months if you do a few simple things like stretching exercises and cutting back on activities that might have caused the problem. Taking over-the-counter medicines can help with pain. It's rare that people need surgery for plantar fasciitis. Doctors only do surgery as a last resort if nothing else eases the pain.
Non Surgical Treatment
Heel cups are used to decrease the impact on the calcaneus and to theoretically decrease the tension on the plantar fascia by elevating the heel on a soft cushion. Although heel cups have been found to be useful by some physicians and patients, in our experience they are more useful in treating patients with fat pad syndrome and heel bruises than patients with plantar fasciitis. In a survey of 411 patients with plantar fasciitis, heel cups were ranked as the least effective of 11 different treatments.

Surgical Treatment
The majority of patients, about 90%, will respond to appropriate non-operative treatment measures over a period of 3-6 months. Surgery is a treatment option for patients with persistent symptoms, but is NOT recommended unless a patient has failed a minimum of 6-9 months of appropriate non-operative treatment. There are a number of reasons why surgery is not immediately entertained including. Non-operative treatment when performed appropriately has a high rate of success. Recovery from any foot surgery often takes longer than patients expect. Complications following this type of surgery can and DO occur! The surgery often does not fully address the underlying reason why the condition occurred therefore the surgery may not be completely effective. Prior to surgical intervention, it is important that the treating physician ensure that the correct diagnosis has been made. This seems self-evident, but there are other potential causes of heel pain. Surgical intervention may include extracorporeal shock wave therapy or endoscopic or open partial plantar fasciectomy.
What May Cause Pain In The Heel To Flare Up

Overview
The plantar fascia is a thick fibrous band that runs the length of the sole of the foot. The plantar fascia helps maintain the complex arch system of the foot and plays a role in one's balance and the various phases of gait. Injury to this tissue, called plantar fasciitis, is one of the most disabling running injuries and also one of the most difficult to resolve. Plantar fasciitis represents the fourth most common injury to the lower limb and represents 8 -10% of all presenting injuries to sports clinics (Ambrosius 1992, Nike 1989). Rehabilitation can be a long and frustrating process. The use of preventative exercises and early recognition of danger signals are critical in the avoidance of this injury.
Causes
Factors which may contribute to plantar fasciitis and heel spurs include a sudden increase in daily activities, increase in weight (not usually a problem with runners), or a change of shoes. Dramatic increase in training intensity or duration may cause plantar fasciitis. Shoes that are too flexible in the middle of the arch or shoes that bend before the toe joints will cause an increase in tension in the plantar fascia. Even though you may have run in shoes that are flexible before, now that you have developed plantar fasciitis, make certain that your shoe is stable and does not bend in the midfoot. Check and be certain that your shoes are not excessively worn. Shoes that do not sufficiently control excessive pronation combined with an increase in training can lead to this condition. A change in running style or parameters, such as starting speed work, running on the ball of your foot or sudden increase in hill workouts may lead to problems. All changes should be gradual and not abrupt. Gait changes such as altering your foot strike, switching shoe style, running barefoot or in minimalist shoes should all be made gradually and not abruptly. The "terrible too's" of too much, too soon, too often with too little rest also applies to "too many changes with too little adaptation". Make your changes gradually and allow your muscles, bones, and other body structures to adapt to the alterations you may be attempting.
Symptoms
Plantar fasciosis is characterized by pain at the bottom of the heel with weight bearing, particularly when first arising in the morning; pain usually abates within 5 to 10 min, only to return later in the day. It is often worse when pushing off of the heel (the propulsive phase of gait) and after periods of rest. Acute, severe heel pain, especially with mild local puffiness, may indicate an acute fascial tear. Some patients describe burning or sticking pain along the plantar medial border of the foot when walking.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Sometimes physical therapy modalities are helpful. The most frequently used modalities include ultrasound (high frequency sound vibrations that create a deep heat and reduce inflammation) and galvanic electrical stimulation ( a carefully applied intermittent muscular stimulation to the heel and calf that helps reduce pain and relax muscle spasm, which is a contributing factor to the pain). This treatment has been found most effective when given twice a week. Repeated taping and padding is sometimes used. The felt pads that will be strapped to your feet will compress after a few days and must be reapplied. While wearing them they should be kept dry, but may be removed the night before your next appointment. Resistant cases of heel pain caused by plantar fasciitis, heel spurs or cases of stress fracture of the calcaneus often need to be placed in a removable below knee cast boot. It is important to be aware of how your foot feels over this time period. If your foot is still uncomfortable without the strapping, but was more comfortable while wearing it, that is an indication that the treatment should help. Remember, what took many months or years to develop can not be eliminated in just a few days.

Surgical Treatment
When more-conservative measures aren't working, your doctor might recommend steroid shots. Injecting a type of steroid medication into the tender area can provide temporary pain relief. Multiple injections aren't recommended because they can weaken your plantar fascia and possibly cause it to rupture, as well as shrink the fat pad covering your heel bone. Extracorporeal shock wave therapy. In this procedure, sound waves are directed at the area of heel pain to stimulate healing. It's usually used for chronic plantar fasciitis that hasn't responded to more-conservative treatments. This procedure may cause bruises, swelling, pain, numbness or tingling and has not been shown to be consistently effective. Surgery. Few people need surgery to detach the plantar fascia from the heel bone. It's generally an option only when the pain is severe and all else fails. Side effects include a weakening of the arch in your foot.
Stretching Exercises
Calf stretch. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Plantar fascia stretch. This stretch is performed in the seated position. Cross your affected foot over the knee of your other leg. Grasp the toes of your painful foot and slowly pull them toward you in a controlled fashion. If it is difficult to reach your foot, wrap a towel around your big toe to help pull your toes toward you. Place your other hand along the plantar fascia. The fascia should feel like a tight band along the bottom of your foot when stretched. Hold the stretch for 10 seconds. Repeat it 20 times for each foot. This exercise is best done in the morning before standing or walking.
What Exactly Brings About Heel Pain

Overview
To find out where this condition gets its name, we need to look at a specific area of the foot. Your foot is made up of bones, muscles, tendons, and ligaments. The plantar fascia is a relatively inflexible, strong, fibrous band on the bottom of the foot that supports the arch of your foot. Beginning at the heel bone, the plantar fascia extends the length of your foot to connect with your toes at the ball of the foot. When you walk, your weight is distributed across your feet. Any imbalances in the mechanics of your foot and distribution of weight can potentially cause pain. Diseases involving inflammation end with "itis." This explains the name of the condition as being an inflammation of the plantar fascia, thus plantar fasciitis. Repetitive movements such as walking or running stretch the plantar fascia. Because it is not very flexible, this can cause small tears in the fascia, which leads to inflammation and pain. Other factors such as high arches, fallen arches, or a change in the walking surface contribute to the stress placed on the plantar fascia and heel.
Causes
When some people stand/walk/run/jump their own anatomy in their ankle joint is not ‘sturdy’ enough to cope with the needed stabilisation of their ankle joint when they are weight bearing. So, their ankle rotates to find a point of stability. By the shin twisting in and the ankle rotating downwards to the inside (along with your body weight, the power of some muscles, and of course, gravity) a huge amount of stress is applied to the plantar fascia until it is stressed beyond it’s normal limits and it starts to ‘tighten up’. It is this tightening up of the plantar fascia under this stress that causes the damage that in turn leads to pain…eventually.
Symptoms
Symptoms of the plantar fasciitis include a gradual onset of pain under the heel which may radiate into the foot. Tenderness is usually felt under and on the inside of the heel which is initially worse first in the morning but eases as the foot warms up only to return later in the day or after exercise. Stretching the plantar fascia may be painful.
Diagnosis
Your doctor will ask you about the kind of pain you're having, when it occurs and how long you've had it. If you have pain in your heel when you stand up for the first time in the morning, you may have plantar fasciitis. Most people with plantar fasciitis say the pain is like a knife or a pin sticking into the bottom of the foot. After you've been standing for a while, the pain becomes more like a dull ache. If you sit down for any length of time, the sharp pain will come back when you stand up again.
Non Surgical Treatment
The following recommendations are appropriate. Wear shoes with adequate arch support and cushioned heels; discard old running shoes and wear new ones; rotate work shoes daily. Avoid long periods of standing. Lose weight. Stretch the plantar fascia and warm up the lower extremity before participating in exercise. For increased flexibility, stretch the plantar fascia and the calf after exercise. Do not exercise on hard surfaces. Avoid walking barefooted on hard surfaces. Avoid high-impact sports that require a great deal of jumping (eg, aerobics and volleyball). Apply ice for 20 minutes after repetitive impact-loading activities and at the end of the day. Limit repetitive impact-loading activities such as running to every other day, and consider rest or cross-training for nonrunning days.

Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
Prevention
More than with most sports injuries, a little bit of prevention can go a long way toward keeping you free from plantar fasciitis. Here are some tips to follow. Wear supportive shoes that fit you well. When your shoes start to show wear and can no longer give your feet the support they need, it's time to get a new pair. Runners should stop using their old shoes after about 500 miles of use. Have a trained professional at a specialty running store help you find the right pair for your foot type, and then keep your shoes tied and snug when you wear them. Stay in good shape. By keeping your weight in check, you'll reduce the amount of stress on your feet. Stretch your calves and feet before you exercise or play a sport. Ask an athletic trainer or sports medicine specialist to show you some dynamic stretching exercises. Start any new activity or exercise slowly and increase the duration and intensity of the activity gradually. Don't go out and try to run 10 miles the first time you go for a jog. Build up to that level of exercise gradually. Talk to your doctor about getting heel pads, custom shoe inserts, or orthotics to put in your shoes. Foot supports can help cushion your feet and distribute your weight more evenly. This is especially true for people with high arches or flat feet. Your doctor will be able to tell you if shoe inserts and supports might lower your chances of heel injury.